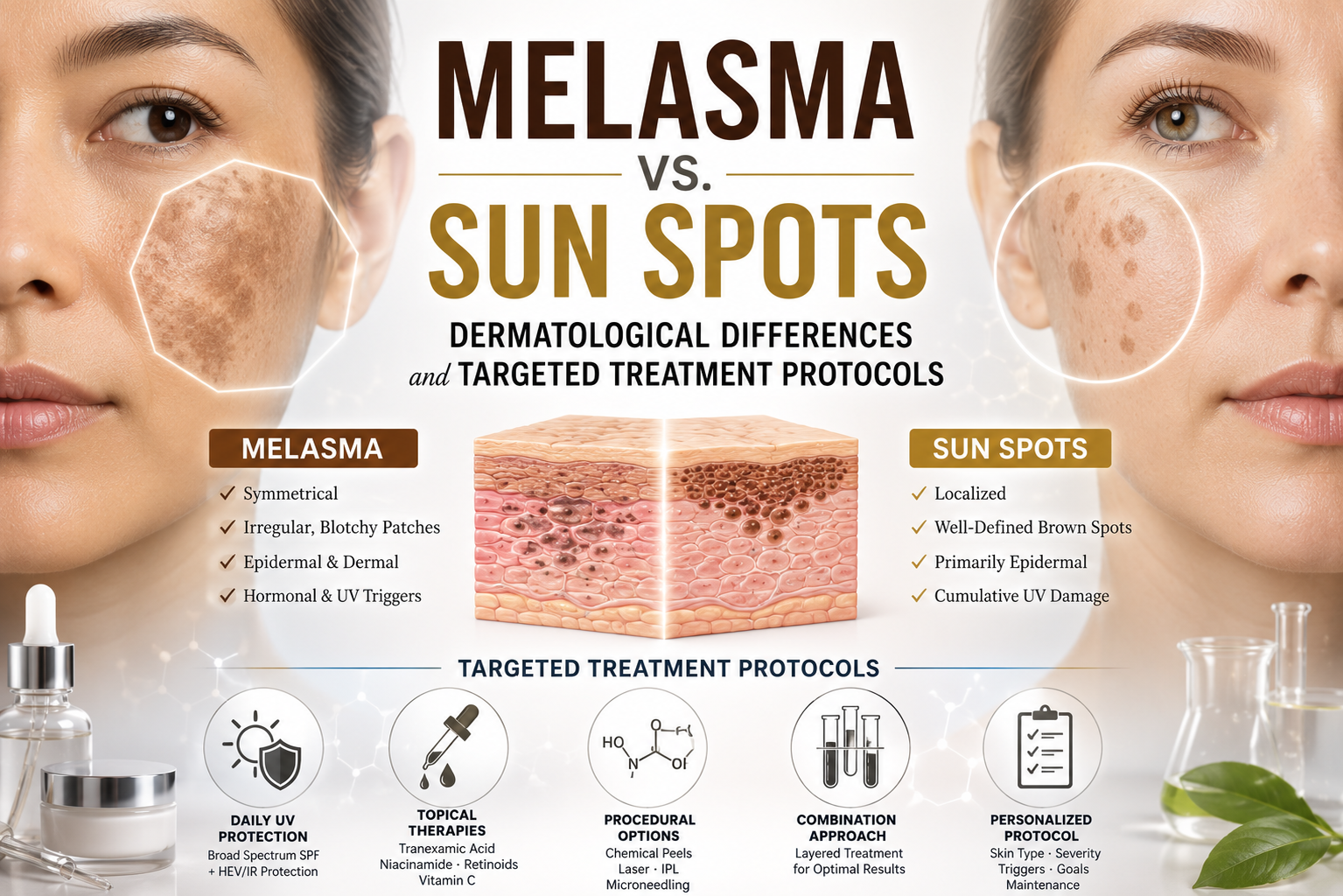
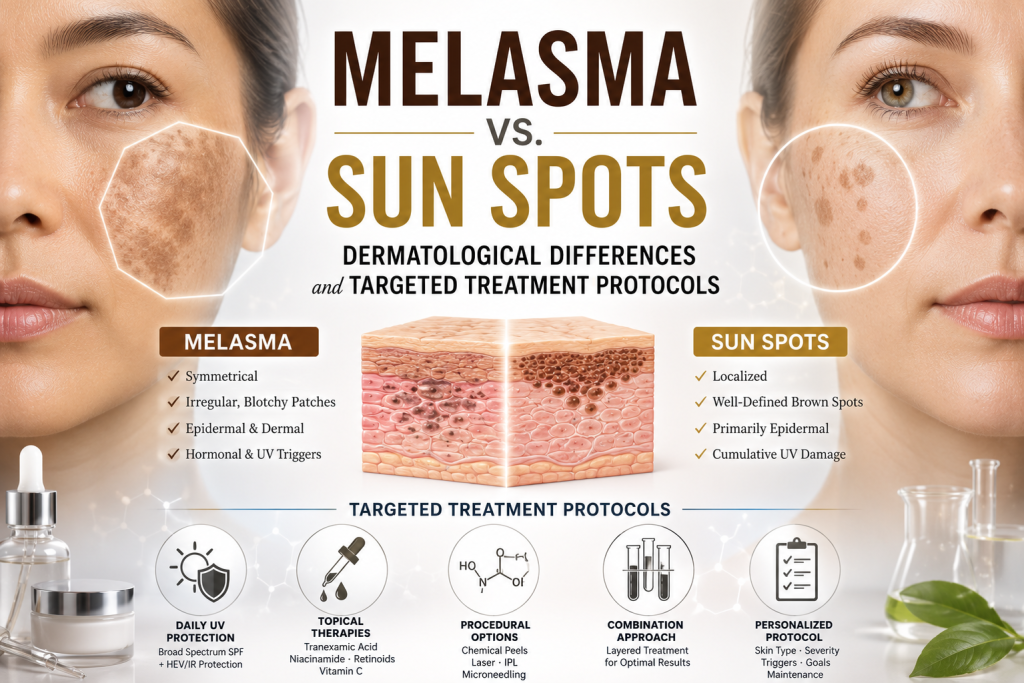
Melasma vs. Sun Spots: Dermatological Differences and Targeted Treatment Protocols
Executive Summary
In the global aesthetic and cosmeceutical market, hyperpigmentation remains one of the most persistent and highly funded consumer concerns. However, a significant portion of skincare investments yields poor returns due to a fundamental diagnostic error: conflating melasma with sun spots. While both conditions manifest as dark patches on the skin, their etiology, depth, and cellular behavior are entirely distinct. For dermatologists, aesthetic practitioners, and consumers seeking clinical-grade results, distinguishing between these two forms of hyperpigmentation is not merely semantic—it dictates the entire therapeutic protocol. Misdiagnosing melasma as a simple sun spot and applying the wrong modality can trigger severe, permanent darkening.
The Pathology of Hyperpigmentation: Two Distinct Pathways
Hyperpigmentation occurs when melanocytes (the skin’s pigment-producing cells) enter a state of hyperactivity, depositing excess melanin into the epidermis or dermis. The critical difference between melasma and sun spots lies in what is stimulating these cells.
1. Sun Spots (Solar Lentigines): The Photodamage Footprint Sun spots, clinically known as solar lentigines or “liver spots,” are the direct result of cumulative, localized ultraviolet (UV) exposure.
- The Trigger: Years of unprotected sun exposure cause melanocytes in specific areas to multiply and cluster, creating a concentrated pool of pigment.
- Visual Characteristics: They appear as distinct, well-defined, flat, light-to-dark brown macules. They are typically asymmetrical and scattered randomly.
- Location: Found exclusively on areas frequently exposed to the sun: the face, the backs of the hands, the décolletage, and the shoulders.
- Depth: Sun spots are generally superficial, residing entirely within the upper layers of the epidermis.
2. Melasma: The Hormonal Network Melasma is a vastly more complex, chronic condition. It is a hyper-melanosis driven by a combination of internal systemic factors and external triggers.
- The Trigger: The primary catalysts are hormonal fluctuations—specifically estrogen and progesterone surges related to pregnancy, oral contraceptives, or thyroid dysfunction. Crucially, melasma melanocytes are hypersensitive not just to UV light, but also to visible light and heat.
- Visual Characteristics: It manifests as dense, symmetrical, map-like patches with poorly defined borders.
- Location: Highly specific to the center of the face: the upper lip, the central forehead, the bridge of the nose, and the upper cheeks.
- Depth: Melasma can be epidermal (superficial), dermal (deep within the living tissue), or mixed, making it notoriously difficult to eradicate.
Diagnostic Comparison at a Glance
| Feature | Melasma | Sun Spots (Solar Lentigines) |
|---|---|---|
| Primary Cause | Hormonal shifts, UV light, Heat | Cumulative UV exposure |
| Appearance | Symmetrical, patchy, map-like | Distinct, scattered, well-defined spots |
| Common Locations | Forehead, cheeks, upper lip | Face, hands, chest, shoulders |
| Demographic | Primarily women (ages 20-50) | Anyone with significant sun exposure |
| Response to Heat | Worsens rapidly | Unaffected |
Dermatological Treatment Protocols: A Divergent Strategy
Because their biological drivers are different, the treatment strategies for melasma and sun spots must be fundamentally opposed.
Treating Sun Spots: Eradication and Resurfacing
Sun spots are generally straightforward to treat. Because the pigment is superficial and not driven by active hormones, practitioners can employ aggressive modalities to physically lift and destroy the clustered pigment.
- Light and Laser Therapies: Intense Pulsed Light (IPL) and Q-Switched lasers are highly effective. They target the dark pigment, causing it to shatter, darken temporarily, and slough off within a week.
- Cryotherapy: Liquid nitrogen can be used to freeze and destroy localized pigment cells on the body (like the hands).
- Chemical Peels: Medium-depth peels utilizing Trichloroacetic Acid (TCA) can effectively resurface the epidermal layer, removing solar lentigines.
Treating Melasma: Suppression and Management
Treating melasma requires extreme caution. Applying intense heat (like IPL) or aggressive lasers to melasma will trigger an inflammatory response that causes the hyperactive melanocytes to produce more pigment, leading to severe rebound hyperpigmentation. Melasma cannot be “cured”; it must be chemically managed.
- Tyrosinase Inhibitors: The gold standard is suppressing tyrosinase, the enzyme required to produce melanin. Prescription formulations utilizing Hydroquinone (the clinical benchmark), Tranexamic Acid, Kojic Acid, and Cysteamine are deployed to halt pigment production at the cellular level.
- Low-Fluence Lasers: If lasers are used, they must be “cold” or low-energy, such as Nd:YAG lasers, which gently break up pigment without generating the heat that exacerbates melasma.
- Strict Heat and Light Avoidance: Patients must utilize mineral sunscreens containing Iron Oxides to block visible light, and actively avoid environments that raise facial core temperature (e.g., saunas, hot yoga).
Conclusion: The Bottom Line for Skincare Investment
In aesthetic medicine, an inaccurate diagnosis is an expensive mistake. Investing in an aggressive laser package for what you believe are “sun spots” on your upper lip could permanently worsen underlying melasma. For consumers and industry professionals alike, achieving a clear, even complexion requires recognizing that sun spots are a superficial footprint of the past, while melasma is an active, hormonal engine. A clinical consultation to establish the correct etiology is the indispensable first step before allocating capital toward any hyperpigmentation protocol.