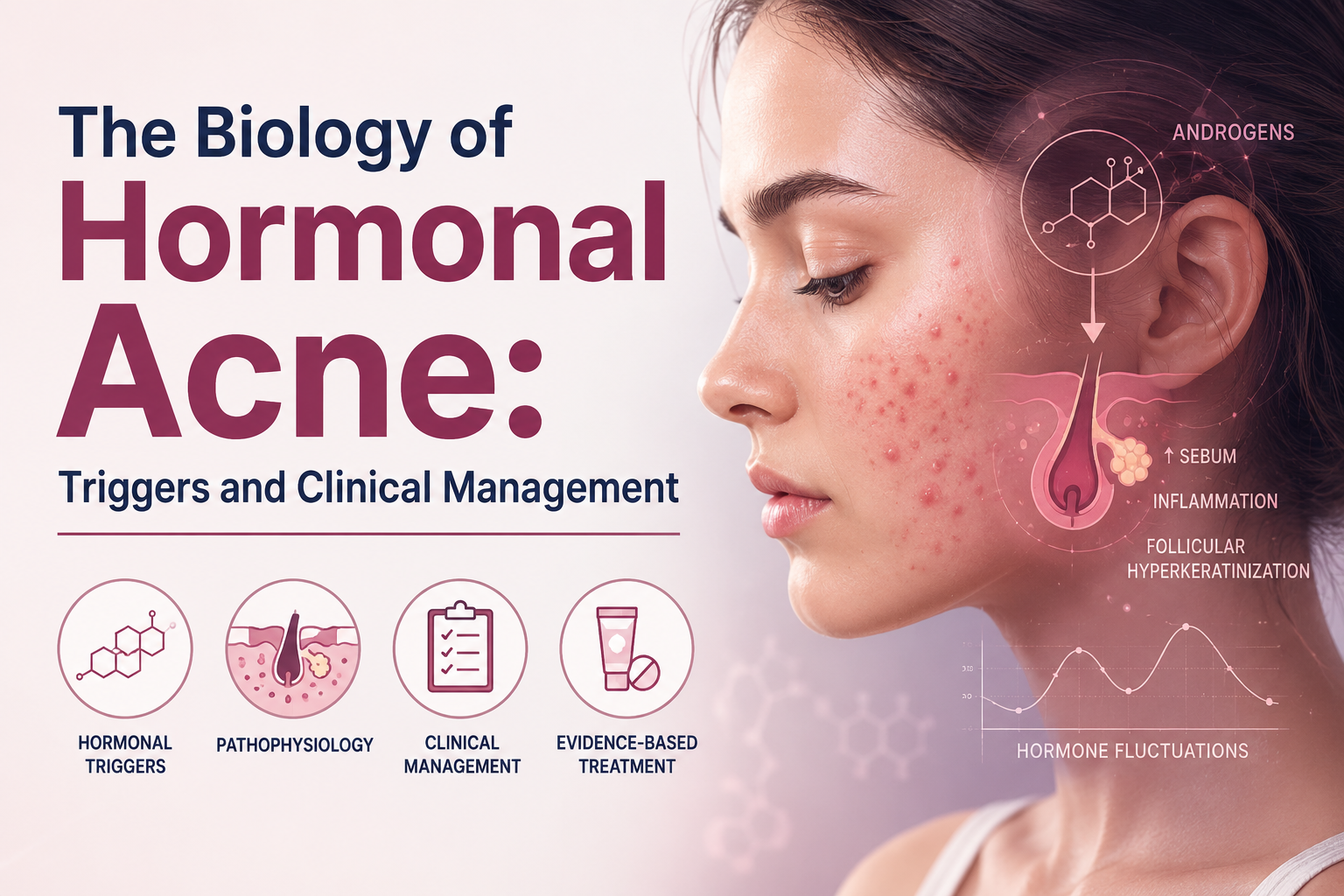
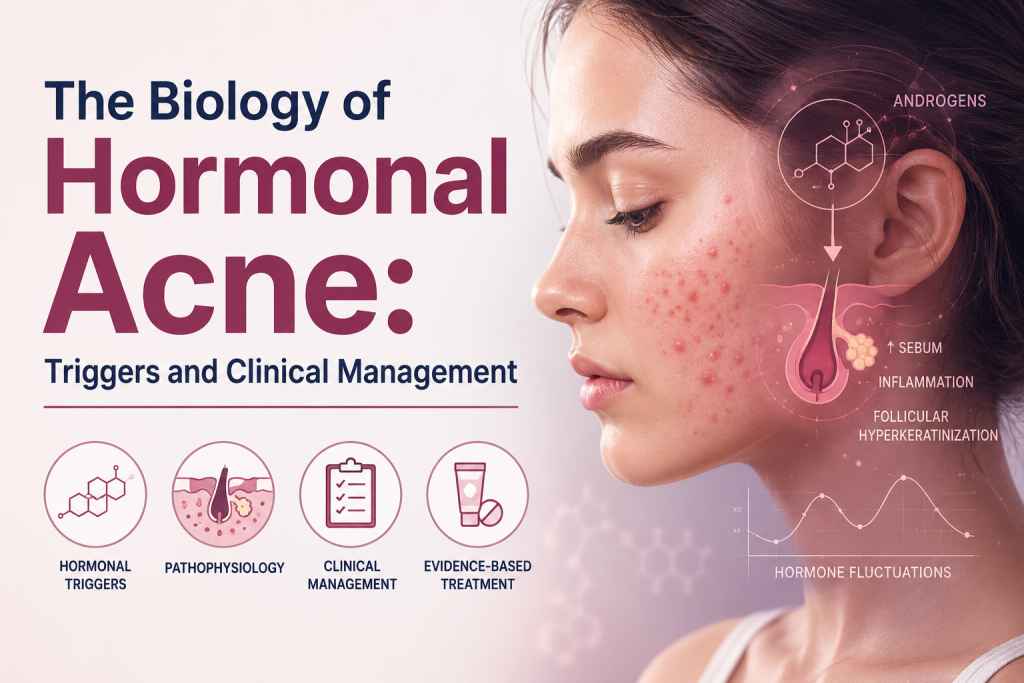
The Biology of Hormonal Acne: Triggers and Clinical Management
For many adults, particularly female professionals, the persistence of acne well beyond adolescence is both a clinical frustration and a psychological burden. Unlike the transient breakouts of puberty, adult-onset acne is deeply rooted in the complex endocrine ecosystem. To effectively treat it, we must move beyond surface-level aesthetics and approach the condition through the rigorous lens of dermatological science.
Here, we decode the biological underpinnings of hormonal acne, identify its primary triggers, and outline evidence-based strategies for clinical management.
Decoding the Endocrine Ecosystem: The Pathogenesis of Hormonal Acne
Hormonal acne is fundamentally a disease of the pilosebaceous unit, driven by systemic endocrine fluctuations. The primary biological culprits are androgens—male sex hormones such as testosterone and its highly potent derivative, dihydrotestosterone (DHT), which are present in both men and women.
When androgen receptors in the skin are overly sensitive, or when there is an absolute increase in circulating androgens, the sebaceous glands go into overdrive. This hyperseborrhea alters the skin’s lipid profile, creating an anaerobic environment where Cutibacterium acnes (C. acnes) thrives. The resulting bacterial colonization triggers a cascade of inflammatory cytokines, culminating in the deep, tender, and cystic nodules classically distributed along the jawline, chin, and lower face.
Understanding this pathogenesis is critical: topicals that merely exfoliate the surface will fail to address the receptor-level dysfunction driving the disease.
Identifying the Catalysts: Primary Biological Triggers
While genetics dictate the sensitivity of your androgen receptors, environmental and physiological factors serve as the catalysts. For modern professionals, these triggers are often deeply intertwined with lifestyle.
- Chronic Cortisol Elevation (Stress): The adrenal glands produce both cortisol (the stress hormone) and DHEA-S (an androgen). Chronic, high-level occupational stress elevates cortisol, which simultaneously increases systemic inflammation and androgen production, leading to stress-induced inflammatory breakouts.
- The Menstrual Cycle: The predictable drop in estrogen and progesterone just before menstruation leaves androgens relatively dominant. This hormonal imbalance is why up to 85% of adult women experience premenstrual flare-ups.
- Dietary Inflammatories (IGF-1): High-glycemic-index foods and certain dairy products stimulate the production of Insulin-like Growth Factor 1 (IGF-1). IGF-1 not only amplifies androgen synthesis but also directly stimulates sebocyte proliferation, worsening follicular hyperkeratinization (the clogging of pores).
Strategic Clinical Management: A Targeted Approach
Effective clinical management of hormonal acne requires a strategic, multi-modal intervention. Rather than reacting to individual lesions, modern dermatological protocols aim to suppress the underlying hormonal cascade and manage localized inflammation.
1. First-Line Topicals: Retinoids and Anti-Androgens
For mild to moderate cases, topical therapy remains foundational. Topical retinoids (such as Tretinoin or Adapalene) accelerate cell turnover, preventing the initial microcomedone formation.
Recently, the dermatological landscape has been revolutionized by topical anti-androgens like Clascoterone (Winlevi). By competitively binding to androgen receptors directly within the sebaceous gland, it blocks DHT from triggering oil production, offering a highly targeted, localized hormonal treatment without systemic side effects.
2. Systemic Interventions: Oral Therapeutics
When topicals are insufficient, systemic management is required to recalibrate the endocrine environment.
- Spironolactone: Originally a blood pressure medication, this oral anti-androgen is highly efficacious for female hormonal acne. It blocks androgen receptors and inhibits 5-alpha-reductase, the enzyme responsible for converting testosterone to the more potent DHT.
- Combined Oral Contraceptives (COCs): FDA-approved COCs reduce circulating free testosterone by increasing Sex Hormone Binding Globulin (SHBG) in the liver. This “binds up” the excess hormones before they can interact with the skin.
3. Adjunctive Modalities
In-office procedures offer excellent adjunctive support. Chemical peels (Salicylic or Mandelic acid) provide lipophilic exfoliation that penetrates the lipid-rich environment of the pore. Additionally, broad-band light (BBL) and targeted laser therapies can directly reduce C. acnes populations and suppress localized vascular inflammation.
The Future: Decoding Skincare Through Science
Treating hormonal acne is not a cosmetic endeavor; it is a clinical practice requiring patience, precision, and an understanding of human biochemistry. As dermatological science advances, the shift is moving away from generalized antibiotics and harsh drying agents toward highly specific, receptor-level therapeutics.
By understanding your unique hormonal triggers and partnering with a clinical professional to design a targeted regimen, you can regain control over your skin’s biological narrative.